
How female hair loss happen?
Unlike hair loss in men, female scalp hair loss may commonly begin at any age through 50 or later, may not have any obvious hereditary association, and may not occur in a recognizable “female-pattern alopecia” of diffuse thinning over the top of the scalp. A woman who notices the beginning of hair loss may not be sure if the loss is going to be temporary or permanent—for example, if there has been a recent event such as pregnancy or illness that may be associated with temporary hair thinning.
In women as in men, the most likely cause of scalp hair loss is androgenetic alopecia—an inherited sensitivity to the effects of androgens (male hormones) on scalp hair follicles. However, women with hair loss due to this cause usually do not develop true baldness in the patterns that occur in men—for example, women rarely develop the “cue-ball” appearance often seen in male-pattern androgenetic alopecia.
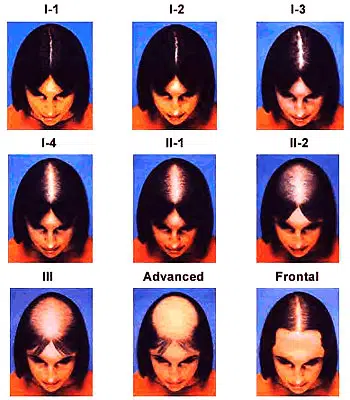
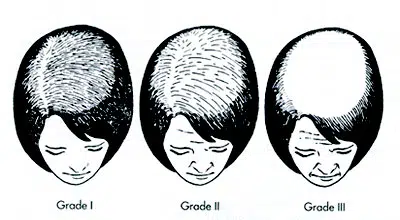
Patterns of female androgenetic alopecia can vary considerably in appearance. Patterns that may occur include (See below pictures):
- Diffuse thinning of hair over the entire scalp, often with more noticeable thinning toward the back of the scalp.
- Diffuse thinning over the entire scalp, with more noticeable thinning toward the front of the scalp but not involving the frontal hairline.
- Diffuse thinning over the entire scalp, with more noticeable thinning toward the front of the scalp, involving and sometimes breaching the frontal hairline.
It is important to note that female pattern hair loss can begin as early as the late teens to early 20s in women who have experienced early puberty. If left untreated, this hair loss associated with early puberty can progress to more advanced hair loss if it is left untreated.
Non-Pattern Causes of Hair loss in Women
In women more often than in men, hair loss may be due to conditions other than androgenetic alopecia. Some of the most common of these causes are:
- Alopecia Areata
- Traction Alopecia
- Scarring Alopecia
- Trichotillomania
- Anagen Effluvium
- Telogen Effluvium
Triangular Alopecia
The cause of triangular alopecia is not known, but the condition can often be treated medically or surgically. The characteristic pattern of hair loss in triangular alopecia is thinning or complete loss of hair in the scalp area around the temples. If hair loss is not complete, the remaining hairs are often “miniaturized”-fine-textured hairs of thin diameter. Triangular alopecia sometimes begins in childhood with unexplained hair loss in the temporal areas of the scalp.
Loose-Anagen Syndrome
Loose-anagen syndrome occurs most frequently in fair-haired persons. During the anagen (growth) cycle of hair, scalp hairs sit so loosely in the follicles from which they grow that they can be easily extracted by combing or brushing. The condition may appear in childhood and gradually improve or disappear over time.
Post-natal alopecia
Postpartum alopecia is properly the most commonly recognized form of telogen hair shedding. During pregnancy there is a progressive increase in the percentage of anagen scalp hairs, 95 percent anagen and 5 percent telogen hair during both the second and third trimesters. This compared with 84 percent anagen in nonpregnant women. Following delivery, there is a rapid decrease in the percentage of anagen hairs, with an associated increase in the percentage of telogen hairs. Hair shedding begins from less than a month to 4 months post partum and may last as long as year, although typically the duration of shedding is less than 6 months. The majority of affected women have a return to normal hair density, unless they have associated female pattern hair loss, in which case regrowth may not return scalp hair density to pre-pregnancy levels. It is widely thought that the high estrogen levels of pregnancy are responsible for prolongation of the anagen phase of the follicular cycle. Additional factors that may be relevant to postpartum hair loss may include stress, blood loss, and other hormonal factors such as prolactin secretion with nursing.
If you are a woman with thinning or lost scalp hair, your first necessary step is to have the condition correctly diagnosed by a physician hair restoration specialist. After a diagnosis is made, the physician will recommend an approach to effective medical or surgical treatment.
Diagnosis
Hair loss in women isn’t always as straightforward as it is in most men. In men about 90 percent of all cases are caused by hereditary male pattern baldness. In women however hair loss can be triggered by a multitude of conditions and circumstances.
The below diagnostic tests should be performed when attempting to pinpoint the hair loss trigger. These tests can at the very least eliminate the possibility of certain disorders causing your hair loss and perhaps find the actual cause. The truth of the matter is that for many patients these test usually come back with reading within the “normal range, but it’s important to remember that the proper diagnosis of female hair loss usually starts of with the process of elimination.
Diagnostic Tests
- Hormone levels (DHEAs, testosterone, androstenedione, prolactin, follicular stimulating hormone, and leutinizing hormone)
- Serum iron
- Serum ferritin
- Total iron binding capacity (TIBC)
- Thyroid stimulating hormone (T3, T4, TSH)
- VDRL (a screening test for syphilis)
- Complete blood count (CBC)
- Scalp biopsy
A small section of scalp usually 4mm in diameter is removed and examined under a microscope to help determine the cause of hair loss. - Hair pull
The hair pull test is a simple diagnostic test in which the physician lightly pulls a small amount of hair (approx 100 simultaneously) in order to determine if there is excessive loss. Normal range is one to three hairs per pull. - Densitometry
The densitometer is a handheld magnification device which is used check for miniaturization of the hair shaft.
Treatment
Hair transplantation in women
Medical treatment
The best results from treatment happen when you begin treatment as soon as possible after the hair loss begins because prolonged androgenetic alopecia may destroy many of the hair follicles. The use of anti-androgens after prolonged hair loss will at least help prevent further hair loss and encourage some hair regrowth from those follicles that have been dormant but are still viable, stopping treatment will result in the hair loss resuming if the androgens aren’t kept in check in some other way. Maintaining your vitamin and mineral levels helps while you’re on anti-androgen medications.
As always, treatments have the best chance of being effective if they are geared to the cause of the hair loss as well as to triggering hair growth.
Currently there is only one FDA approved treatment for female pattern hair loss.
Below you will find a list of treatments currently being used to treat hair loss in women. Some of these drugs have not been approved by the FDA for this particular application, however they have all been approved for other applications and are used “off label” to treat hair loss.
The effectiveness of these agents and methods vary from person to person, but many women have found that using these treatments have made a positive difference in their hair and their self-esteem.
Minoxidil 2% Topical Treatment.
Women with diffuse androgenetic alopecia can use minoxidil and it actually seems to be more effective for women compared to men. The makers of minoxidil recommend women only use the 2% concentration of minoxidil and not 5%. The makers of minoxidil have not received FDA approval for promoting 5% minoxidil or minoxidil extra strength for use by women. Many dermatologists do prescribe minoxidil 5% for women with androgenetic alopecia if used under their supervision. Some small clinical trials have been conducted on 5% minoxidil for androgenetic alopecia in women showing that indeed the 5% solution is significantly more effective in both retaining and regrowing hair than the 2 % solution.
Androgen Receptor Inhibitors
Aldactone / Spironolactone
Spironolactone is an antiandrogen that works in two ways. Primarily it slows down the production of androgens in the adrenal glands and ovaries. Secondly it blocks the action of androgens in part by preventing dihydrotestosterone from binding to its androgenetic receptor.
Tagamet / Cimetidine
Cimetidine has a fairly powerful anti-androgenic effect and has shown to block dehydrotestosterone form binding the follicle receptor sites.
Cyproterone Acetate
Cyproterone Acetate is used to reduce sex drive in men which have excessive sex drive and for the treatment of pronounced sexual aggression. It is also prescribed to treat severe hirsuitism in woman of childbearing age and also androgenetic alopecia in women. Cyproterone acetate exerts its effects by blocking the binding of DHT dihydrotestosterone to its receptors.
Estrogen/Progesterone
Also known as hormone replacement therapy (HRT) and commonly prescribed at menopause, estrogen and progesterone pills and creams are probably the most common systemic form of treatment for androgenetic alopecia for women in menopause or whose estrogen and/or progesterone are lacking for other reasons.
Oral Contraceptives
Since birth control pills decrease the production of ovarian androgens, they can be used to treat women’s androgenetic alopecia.
Nizoral/Ketoconazole
It has anti-androgenic effects and can cause a reduction in the production of testosterone and other androgens by the adrenal gland and by the male and female reproductive organs (in women, the ovaries). Because of this action, it can be used to help treat hair loss. Nizoral shampoo contains 2 percent Ketoconazole and is prescribed not only for the treatment of scalp conditions, but also in combination with other treatments for androgenetic alopecia.
Cyproterone Acetate with Ethinyloestradiol
Sold under the brand name Diane 35 and Diane 50, this contraceptive tablet is prescribed in Europe for women’s androgenetic alopecia. The drug works by blocking some of the actions of male hormones commonly present in women. Although it’s possible for the drug to stop further hair loss and trigger regrowth of hair within about a year, it needs to be used on an ongoing basis in order to maintain regrowth and eliminate hair loss.