Surgical Plan for Class VI–VII Hair Loss
Comprehensive Strategy for Advanced Male Pattern Baldness
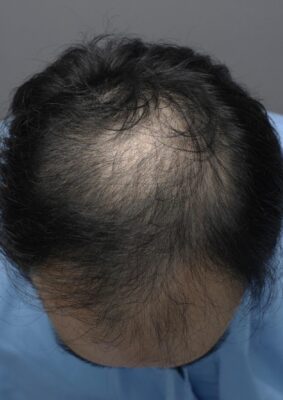
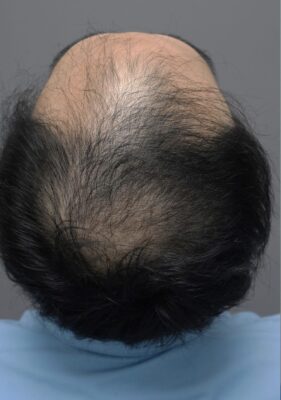
Norwood Class VI–VII hair loss represents the most advanced stages of androgenetic alopecia, characterized by extensive loss of the frontal, mid-scalp, and vertex zones with persistence of only a narrow occipital and parietal horseshoe fringe. Surgical hair restoration in these cases requires meticulous planning, realistic goal-setting, and long-term strategy to maximize limited donor resources.
This article outlines a structured approach to evaluating and designing a surgical plan for Class VI–VII patients.


////////////////////////////////////////////////////////////////////


—
1. Patient Evaluation
1.1 History & Expectations
Age, progression rate, family history
Prior medical treatments (finasteride, dutasteride, minoxidil)
Scalp laxity, donor miniaturization
Patient’s target hairstyle and density expectations
Emphasis on lifetime management: realistic density, future loss potential, potential secondary procedures
1.2 Clinical Assessment
Donor density and quality:
Typical safe donor density varies 60–90 FU/cm²; Class VI–VII often have reduced usable zones.


Safe Donor Zone (SDZ):
Vertical and horizontal boundaries must be accurately mapped to avoid harvesting from areas susceptible to future loss.
Hair characteristics:
Caliber, curl, color–skin contrast significantly influence visual density.
—
2. Surgical Goals for Advanced Hair Loss
2.1 Establish a Natural, Age-Appropriate Hairline
Avoid low, youthful hairlines due to inadequate donor supply.
Strategic creation of a mid-frontal forelock and conservative temporal shape to provide strong framing without compromising resources.
2.2 Achieve Coverage, Not Cosmetic Density Everywhere
Full density across the entire balding area is impossible.
Priority zones:
1. Frontal third (primary cosmetic region)
2. Mid-scalp (secondary)
3. Crown (tertiary) – often reduced density or pattern restoration only.
2.3 Optimize Long-Term Donor Management
Ensure graft allocation allows for future touch-ups or refinement procedures.
Consider donor-preserving techniques.
—
3. Donor Harvesting Strategy
3.1 FUE
FUE (Follicular Unit Extraction)
Individual hairs are taken one by one from the back and sides.
No linear scar
Body hair FUE,
beard, chest hair
Often used for advanced hair loss to maximize total grafts
Helps achieve the best possible coverage
3.2 Graft Numbers (Typical Ranges)
While actual yield varies:
Class VI: 5,000–6,000 FU for meaningful frontal + mid-scalp coverage
Class VII: 6,000–7,500+ FU needed for full pattern restoration with crown blending
—
4. Recipient Design and Density Planning
4.1 Frontal Third
Aim for 35–45 FU/cm² depending on donor supply and hair characteristics.
Create macro- and micro-irregularities for natural contour.
Build strong central forelock as the visual anchor.
4.2 Mid-Scalp
Target 25–30 FU/cm², enough to create a seamless transition.
Angulation and direction must follow natural whorls.
4.3 Crown / Vertex
Crown is a density sink; conservative planning required.
Options:
Light coverage (15–20 FU/cm²)
Whorl reconstruction only
Defer crown work until after medical stabilization
—
5. Medical Therapy Integration
Medical treatment is essential in advanced cases to preserve remaining hair and stabilize long-term results.
Recommended:
Oral finasteride or dutasteride
Topical or oral minoxidil
Adjuncts such as LLLT, PRP (case-dependent)


/////////////////////////////////


////////////////////////////////////////////


6. Staged Surgical Approach
Stage 1 (Primary):
Design and transplant frontal and mid-scalp zones
4,000–45,00 grafts (depending on technique and donor capacity)
Stage 2 (Optional, after 12 months):
Density enhancement of frontal/mid-scalp
Crown pattern work
Additional 1,500–2,500 grafts
Stage 3 (As needed):
Minor refinements over following years
—
7. Key Considerations in Class VI–VII Patients
Donor limitations dictate the plan, not patient desires alone.
Overly aggressive hairlines lead to donor depletion.
Crown work must always be conservative.
Long-term perspective is crucial as progressive thinning continues.
Proper hydration, graft handling, and implantation technique directly influence survival rates.
Communication about realistic outcomes prevents postoperative dissatisfaction.
—
Conclusion
Managing Class VI–VII male pattern baldness is one of the most challenging aspects of hair restoration surgery. Success depends on a balanced strategy prioritizing natural appearance, lifetime donor management, and thoughtful density distribution. Through a staged approach, careful donor mapping, and realistic goal-setting, surgeons can provide significant cosmetic improvement even in patients with extensive hair loss.
////////////////////////////////////////

First session 4000 grafts

Second session 2500 grafts for crown area
